
Rohola Zandie , Robert Betancort , Farhan Khodaee
Digital Liver
DILI
Drug Safety
Toxicology
Therapeutic index

DILI-Context: A Dose- and Exposure-Enriched Knowledge Base for Translational Liver Safety Assessment
Abstract
For most of recorded history, people believed life itself lived in the liver. Mesopotamian priests read the future in sheep livers, the Greeks and Romans treated it as the seat of the soul, and in Persian the strongest way to tell someone they matter is still to say you are my liver. Anatomy later moved that symbolic authority to the heart but pharmacology did not. The liver remains the organ on which the safety of nearly every medicine ultimately depends, and it is the one most often implicated when a drug fails or gets pulled from the market.
A recent piece of work from our team makes the case that understanding the liver well enough to predict harm is now a computational problem. It’s a concrete first step toward building a digital liver for assessing drug-induced liver injury (DILI). We share this work in the Toxicological Science journal as a new knowledge base called DILI-Context.
Keywords: Digital Liver, DILI, Drug Safety, Toxicology, Therapeutic Index
Hazard is not the same as risk
Drug-induced liver injury, or DILI, is a leading cause of late-stage drug failure and post-marketing withdrawal. What makes it so hard to predict is that safety issues are not inherent to the molecule and are not fixed in its chemistry. The same latent hazard may never manifest at one dose and cause serious injury at another. Whether harm actually appears depends on how much drug a patient is exposed to, for how long, by what route, and through which metabolic and immune machinery.
That last point matters enormously. The liver's job is biotransformation: converting the compounds we ingest into forms the body can excrete. The enzymes that do this work, dominated by the cytochrome P450 family, are among the most genetically variable traits in humans. Layer on the adaptive immune system, where specific HLA types predispose particular people to injury from particular drugs, and you get a response that is combinatorial. A patient's reaction is a function of their enzyme genotype, their immune genotype, the drug, the dose, and their exposure history all at once.
The tools we lean on today are not sufficient to see the whole picture. Animal studies miss exactly the idiosyncratic, immune-mediated reactions that most often force a drug off the market. Single-cell-type lab assays cannot reproduce the liver's layered tissue architecture and genotypic variations in enzymes and immune system. And most traditional ML models are trained to answer simple hazard questions which do not provide dose-dependent, route-dependent and duration-dependent context of DILI.
Why the benchmarks are flawed
Here is the gap DILI-Context set out to fix. The field's standard reference datasets, such as the widely used DILIst or DILIRank, label drugs by categorical hazard: toxic/not-toxic or most concern/less concern/no concern. These labels are essential for benchmarking, but they encode hazard, not the exposure conditions under which hazard becomes real injury.
Models trained only on those categories tend to drift toward memorizing chemical scaffolds and drug classes rather than learning the dose-and-exposure relationships that actually govern clinical risk. The result is a model that recognizes families of risky-looking molecules without understanding why or when they become dangerous.
What DILI-Context Shows
DILI-Context keeps the human-adjudicated DILIrank labels as a backbone and enriches them with the quantitative layers that safety scientists actually reason about. Working across a minimal version of FDA-approved small molecules, we integrated five major pharmacological and toxicological databases, then used a mix of automated label parsing, machine-learning classifiers, and deterministic harmonizers to extract clinical dose, treatment duration, route of administration, and preclinical toxicity thresholds. All values were normalized to a common footing so that animal doses and human doses could be compared directly.
From that harmonized and standardized resource, several mechanistic patterns emerged.
Higher doses track with higher risk. Median daily doses climbed steadily from the "no concern" category up to the "most concern" category, and this held across every data source. Drugs that need large amounts of active compounds to work tend to expose the liver to more parent drug and reactive metabolite, which fits the observation that safer drugs are often the potent, low-dose ones.
Risky drugs live in narrower safety windows. We computed a Therapeutic Index (the gap between an acutely toxic dose and the clinical dose) and a Margin of Safety (the chronic version of the same idea). Both shrank systematically as DILI concern rose. The most hepatotoxic drugs operate with clinically effective doses sitting close to their toxicity thresholds, leaving little room for patient variability or drug interactions.
Therapeutic Index (Acute Context): Represents the margin of safety against acute overdose or massive necrosis. It is defined as the ratio of the aggregated acute toxicity threshold (HED derived from LD50) to the clinical Defined Daily Dose (DDD).

Margin of Safety (Chronic Context): Represents the margin of safety against cumulative injury or idiosyncratic DILI driven by metabolic stress. It is defined as the ratio of the chronic No Observed Adverse Effect Level (HED derived from NOAEL) to the clinical DDD. Where a NOAEL was unavailable, the Lowest Observed Adverse Effect Level (LOAEL) was used as a conservative proxy.

No-effect thresholds beat lowest-effect thresholds. Chronic no-adverse-effect levels (NOAEL) discriminated risk far better than lowest-adverse-effect levels (LOAEL). This lines up with the mechanistic idea that injury appears not at the first detectable signal, but at the exposure where the liver's compensatory defenses get overwhelmed.
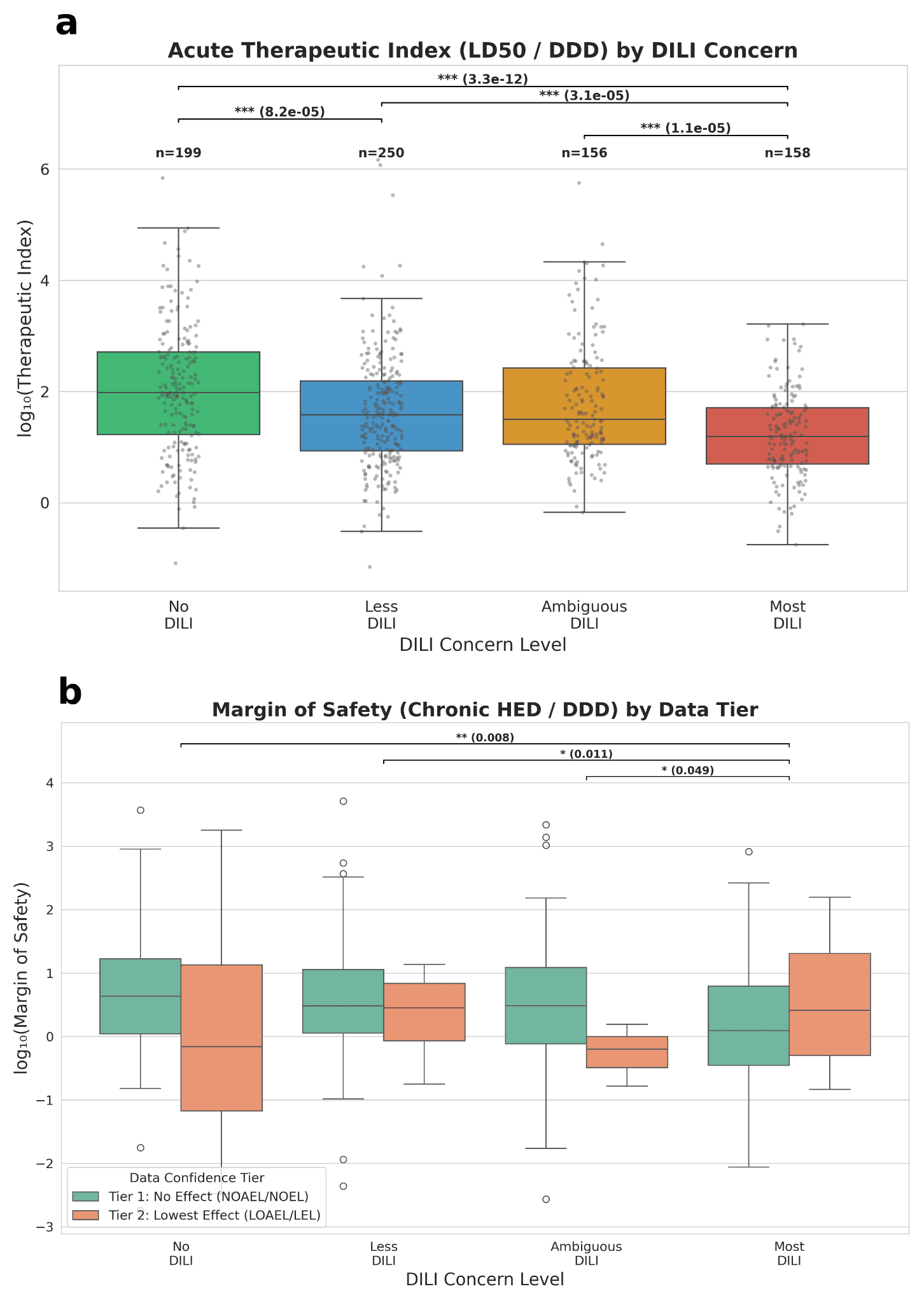
Safety metrics across DILI severity levels. (a) Distribution of Therapeutic Index (TI) values, demonstrating significantly lower TI in drugs with higher DILI concern. (b) Margin of Safety (MoS) for Tier 1 (high-confidence) compounds, showing a trend of lower values associated with increased DILI risk.
Cumulative burden is critical. We introduced a new metric called Chronic Load Score (CLS) that combines dose magnitude with treatment duration. It stratified concern levels cleanly and matched an independent regulatory signal: drugs flagged for hepatic dose adjustment in their prescribing information were heavily concentrated in the high-concern categories, a more than threefold enrichment from the safest to the riskiest tier.
Finally, a compact modeling experiment showed that adding these exposure-derived features to a structure-only classifier improved predictive performance. The gains were incremental, which is expected when looking at a small dataset and only focusing on specific pharmacological class, but they point to real signals beyond structure alone.
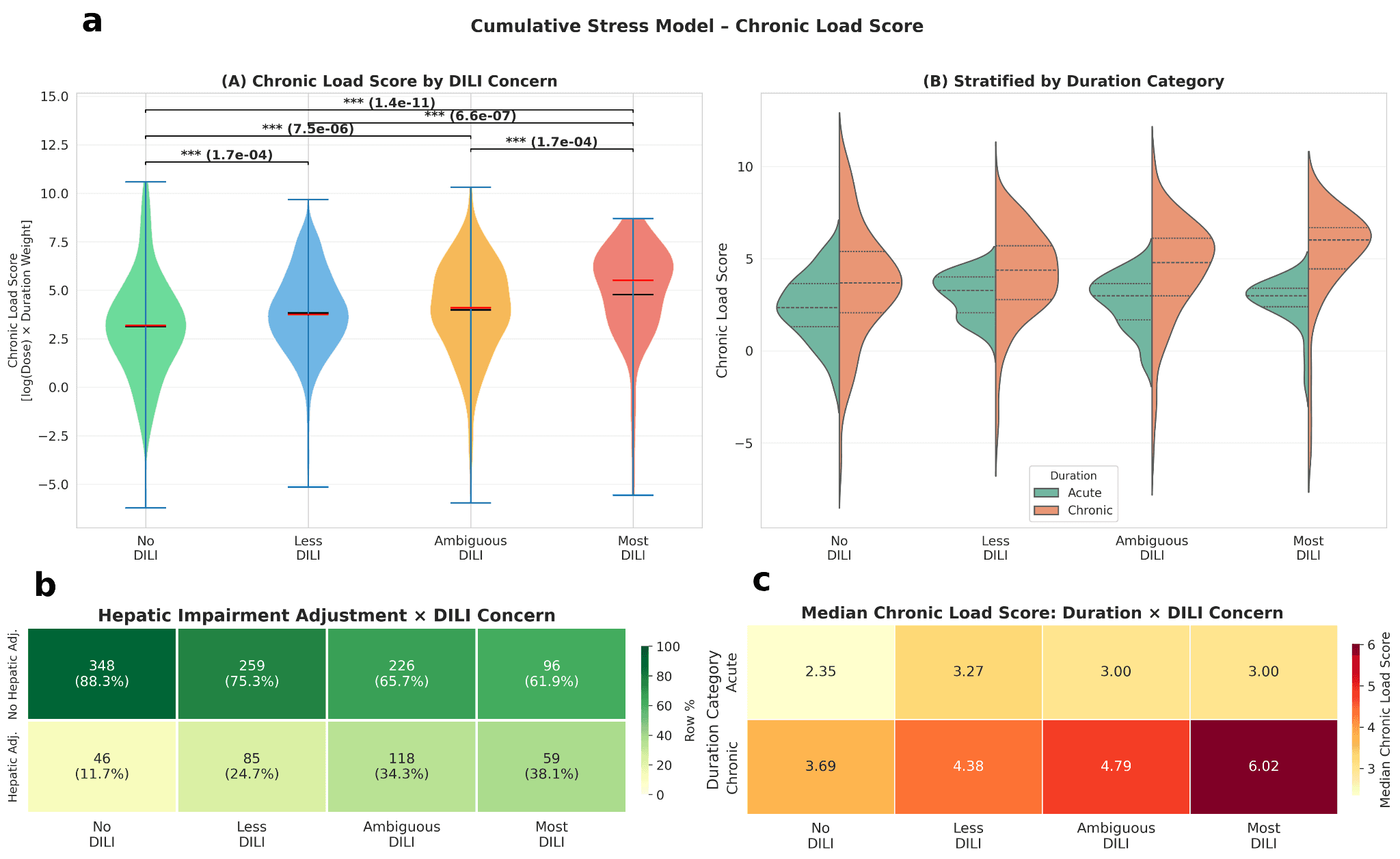
Interaction between treatment duration and chronic hepatic burden. (a) Violin plots illustrating the Chronic Load Score across DILI concern levels, stratified by exposure duration; statistically significant differences are observed across all classes when cumulative exposure is considered (p < 0.05). (b) Annotated heatmap characterizing the association between hepatic impairment dosage adjustments and DILI concern, identifying regulatory dosage labels as a high-confidence signal for toxicity. (c) Heatmap representing the median Chronic Load Score as a function of treatment duration and DILI concern level.
The DILI-Context dataset is the first dose- and exposure-enriched knowledge base for drug-induced hepatotoxicity. We show, through extensive analysis, that therapeutic dose requirements, therapeutic indices, chronic safety margins, and cumulative exposure burdens stratify systematically across DILI concern categories, emphasizes the main idea that clinical hepatotoxicity risk is governed not by intrinsic chemical hazard alone, but by the interplay of hazard and exposure.
From a dataset to a digital liver
DILI-Context is best understood as one component of a larger ambition that we have. We are building a digital liver: a computational twin that couples mechanistic models of hepatic injury, with a data-driven learning layer trained on large drug-response datasets, and grounded experimentally in in-vitro, in-vivo and clinical measurements.
The mechanistic backbone brings causal structure and the ability to reason across multiple layers of complex biology. The learning layer absorbs heterogeneous data and captures mechanisms not yet formalized. Coupled together, it allows us to simulate whole virtual patient populations, sampling realistic distributions of enzyme genotypes, immune risk alleles, and physiology, then estimate what fraction of a population a given molecule would put at risk.
DILI-Context supplies part of the fuel for that machine. By turning categorical hazard labels into context-aware safety maps, it lets models distinguish a potent, low-exposure oncology drug from a low-hazard drug that accumulates risk through years of chronic use. That distinction is exactly what a human safety reviewer makes, and exactly what most current models cannot.
Reframing hepatic safety as an exposure-dependent, computable problem is a concrete step toward medicine that can anticipate, before a drug is ever given, how a particular person's liver will answer it.
Acknowledgement
We would like to thank Dr. Weida Tong of Division of Bioinformatics and Biostatistics, FDA National Center for Toxicological Research (NCTR) for insightful discussions during the preparation of this work.
DILI-Context is now published in Toxicological Sciences. Read the full paper here: https://doi.org/10.1093/toxsci/kfag077
